56 year old man, DKA with right 3rd and 4th Toe amputation
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
56 year old man was posted for amputation of 3rd and 4th toe at 3pm referred to us in view of high blood sugars - 425 mg/dl
He was apparently asymptomatic 3 years back then he was diagnosed to be diabetic when he was taken to a local hospital after the attendants observed that he had lost weight .He has been on insulin mixtard 20 units in the morning and tab metformin 500mg in evening since 2.5 years. He used to work as a farmer but has been at home since 3 years. Used to consumed toddy everyday and also used to smoke around 12 beedis everyday 10 years back
7 days back a bleb was formed on the dorsum of his left foot. He was taken to an RMP practitioner who apparently bursted the bleb and removed the dead skin and came home for dressing everyday. On the 3rd day the attendant noticed small insects in the area and the following day there was discoloration of 3rd and 4th toe. He was brought to our hospital and amputation of 3rd and 4th toe was perfomed. Then he was referred to us in view of high blood sugars.
Day1
He was brought to our hospital and amputation of 3rd and 4th toe was perfomed. Then he was referred to us in view of high blood sugars.


Day 2
He was catheterised and urine for ketone bodies sent which were found out be positive
Blood samples for RFT , CBP , ABG were sent
He was started on Continuous IV fluids and Insulin drip at 3ml/hr
Debridement was done by surgery department







56 year old man
With DKA
Gangrene of right 3rd and 4th toe for which amputation has been done 2 days back
DM type 2 since 3 years
AKI on CKD
Hypoalbuminaemia
No fresh complains
PR at 72 bpm
Bp 100/70mmhg
Afebrile
Cvs - S1,S2
Lungs - clear
Continued him on 3 ml/hr Insulin drip
Morning grbs was 284 mg/dl
Adequate hydration and continuous iv fluids
Inj 2 ampoules of kcl given in 500ml NS slow iv
Currently on INJ metrogyl and augmentin
On protein x powder with egg white supplementation






Day 4
56 year old man
Admitted with
DKA ( resolved)
Right 3rd and 4th toe amputation
AKI on CKD
Hypoalbuminaemia
Patient says
Grbs at 8 am - 260mg/dl
PR - 102 bpm
Bp - 100/70mmhg
Afebrile
Cvs - S1,S2
Lungs clear
Abdomen soft and non tendet
Tapered off Insulin and has been started on subcutaneous insulin
Disarticulation of 5th toe was done
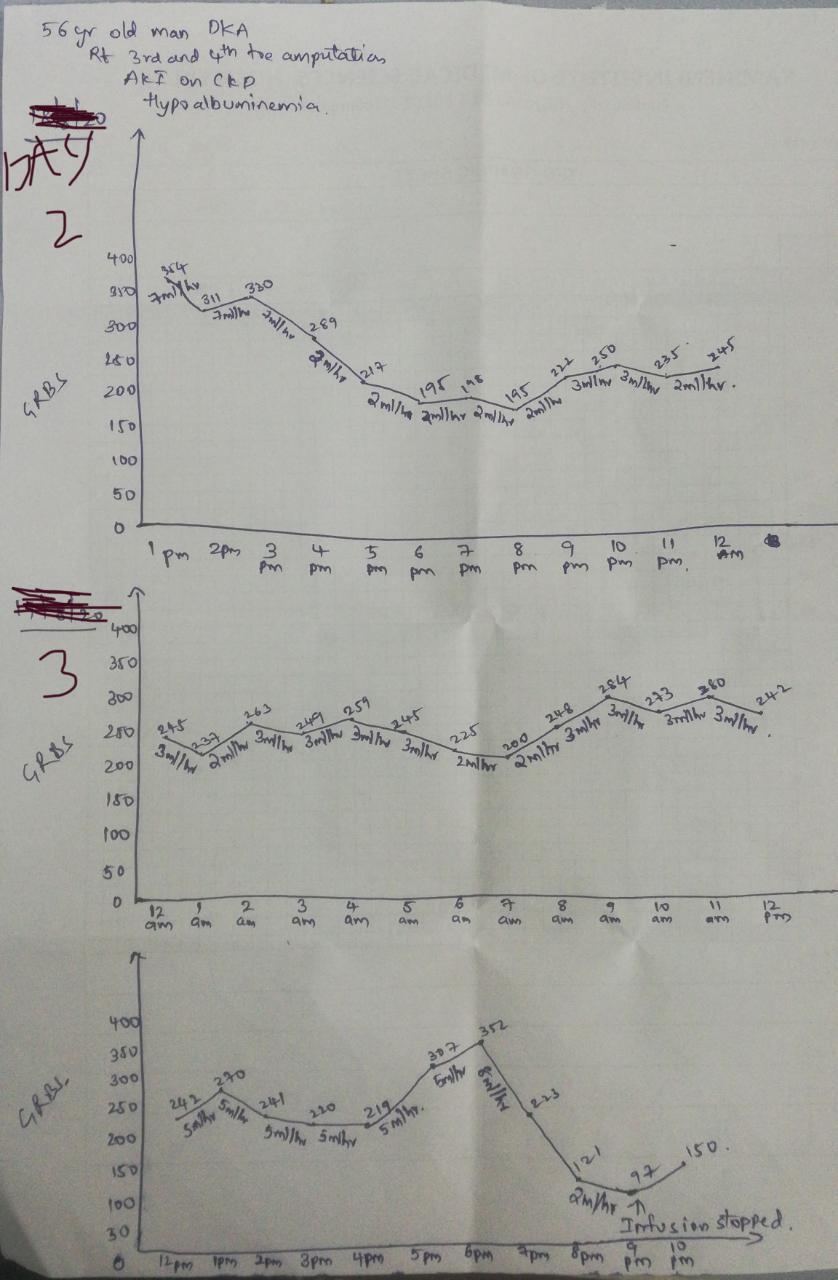
GRBS CHARTING:
Day 5
56 year old man
Admitted with
DKA ( resolved)
Right 3rd and 4th toe amputation
AKI on CKD
Hypoalbuminaemia (secondary to nutritional cause)
Patient says he is feeling better, no fever spikes, stools passed.
Grbs at 8 am - 301mg/dl(dose fixed to 20-20-20 units human actrapid)
Mild pallor and mild icterus present
PR - 100 bpm
Bp - 110/70mmhg
Afebrile
Cvs - S1,S2
Lungs clear
Abdomen soft and non tender

Management of a diabetic ketoacidosis patient:
- Replace fluids : 2-3 litres of 0.9% saline over first 1-3 hr (10-20ml/kg Per hour ); subsequently 0.45% saline at 250-500ml/hr; change to 5% glucose and 0.45% saline at 150-250ml /hr when plasma glucose reaches 250mg/dl (13.9 mmol/litre)
- Administer short acting regular insulin : IV (0.1 units/kg) , then 0.1 units/kg per hour by continuous IV infusion ; increase two to threefold if no response by 2-4 hr . If the initial serum potassium is <3.3 mmol/litre , do not administer insulin until the potassium is corrected.
- Assess patient: what precipitated the episode ( noncompliance , infection, trauma , pregnancy, infarction, cocaine) ?Initiate appropriate workup for precipitating event( cultures, CXR, ECG)
- Measure capillary glucose every 1-2hr ; measure electrolytes ( especially potassium, bicarbonate, phosphate) and anion gap every 4 hr for first 24 hrs.
- Monitor blood pressure, pulse, respirations, mental status, fluid intake and output every 1-4 hr
- Replace potassium: 10meq/hr when plasma potassium <5-5.2 meq/l ( or 20-30 meq/l of infusion fluid ), ECG normal, urine flow and normal creatinine documented; administer 40-80 meq/hr when plasma potassium < 3.5 meq/l or if bicarbonate is given. If initial serum potassium is >5.2 meq/l, do not supplement potassium until potassium is corrected.
- Continue bicarbonate and phosphate supplementation until patient is stable , glucose goal is 8.3-11.1 mmol/l( 150-200mg/dl) and acidosis is resolved. Insulin infusion may be decreased to 0.02-0.1units/kg per hour
- Administer long acting insulin as soon as patient is eating. Allow for a 2-4 hr overlap in insulin infusion and subcutaneous long acting insulin injection.
From Harrison 20th Edition


Comments
Post a Comment